
Overview
Blood Supply of the Brain
The brain is supplied by paired internal carotid arteries and vertebral arteries. The vertebral arteries arise from the subclavian arteries and join to form the basilar artery. Spinal arteries and the posterior inferior cerebellar artery develop from the vertebral arteries before the 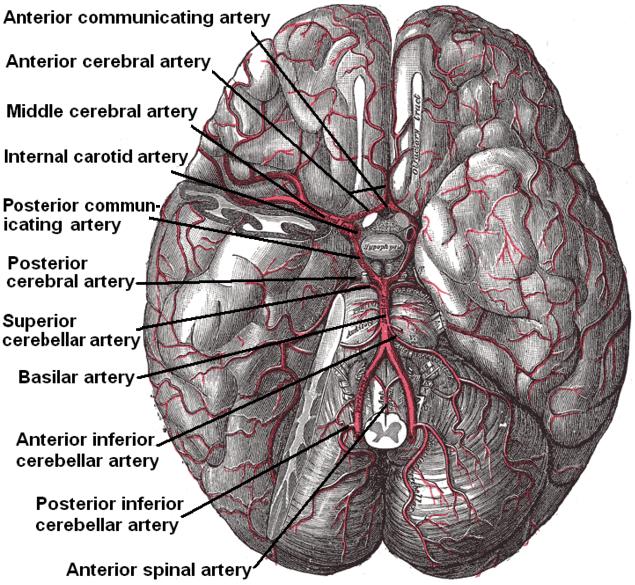 basilar artery is formed. The basilar artery runs the length of the pons and eventually divides into the superior cerebellar arteries and the posterior cerebral arteries. Before this the anterior inferior cerebellar arteries branches off, which supplies the anterior inferior part of the cerebellum. The posterior cerebral artery curves round the midbrain to supply the visual cortex and part of the temporal lobe. The posterior communicating arteries join the posterior cerebral arteries to the internal carotid arteries and the middle cerebral arteries. The internal carotid artery arises from the common carotid artery and divides into its two terminal branches, the anterior and middle cerebral arteries. The anterior communicating artery joins the two anterior cerebral arteries which eventually completes what is known as the Circle of Willis. The middle cerebral artery and the basilar artery however are not considered part of the Circle of Willis.
basilar artery is formed. The basilar artery runs the length of the pons and eventually divides into the superior cerebellar arteries and the posterior cerebral arteries. Before this the anterior inferior cerebellar arteries branches off, which supplies the anterior inferior part of the cerebellum. The posterior cerebral artery curves round the midbrain to supply the visual cortex and part of the temporal lobe. The posterior communicating arteries join the posterior cerebral arteries to the internal carotid arteries and the middle cerebral arteries. The internal carotid artery arises from the common carotid artery and divides into its two terminal branches, the anterior and middle cerebral arteries. The anterior communicating artery joins the two anterior cerebral arteries which eventually completes what is known as the Circle of Willis. The middle cerebral artery and the basilar artery however are not considered part of the Circle of Willis.
Image courtesy of wikimedia commons in the public domain and is thus free of any copyright licence.
The blood supply can also be split up into two parts:
The Anterior Circulation and the Posterior Circulation.
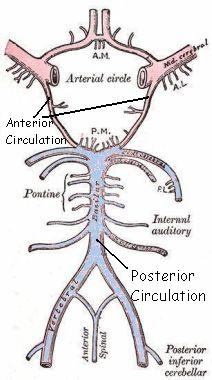
Anterior Circulation
Large Vessels: Internal Carotid Artery, Middle Cerebral Artery, Anterior Cerebral Artery
Small Vessels: Branches from Middle Cerebral Artery and Anterior Cerebral Artery
Posterior Circulation
Large Vessels: Vertebral Arteries, Basilar Artery, Posterior Cerebral Artery
Small Vessels: Branches from the large vessels
Anterior Circulation supplies anterior 2/3 of cerebrum
Posterior Circulation supplies occipital lobe, brain stem and cerebellum.
Image courtesy of wikimedia commons in the public domain and is thus free of any copyright licence.
Stroke Categories
- Total anterior circulation stroke
- Partial anterior circulation stroke
- Posterior circulation stroke
- Lacunar stroke
Total Anterior Circulation Stroke
A total anterior stroke can arise from complete middle cerebral artery infarct, internal carotid disease or intracranial haemorrhage. The patient can be drowsy with hemiparesis affecting the arm face and leg. There is complete aphasia if the dominant hemisphere is affected and the patient may be incontinent. These strokes carry a high mortality with survivors usually have a long term disability.
Partial Anterior Circulation Stroke
A partial anterior circulation stroke occurs when there is infarction in a branch of the middle cerebral artery. This can produce different combinations of problems depending on the affected area. Common deficits include Wernicke’s and Broca’s aphasia with distal branch infarcts leading to weakness of one limb. An anterior cerebral artery infarct usually produces a hemiparesis of the leg with mixed aphasia or dyspraxia (impairment in the performance of an action).
Posterior Circulation Stroke
Occlusion of the basilar artery can lead to lesions in both posterior cerebral arteries and brain stem lesions preventing the conscious part of the brain having any control over movements, although some eye movements may still remain. Infarction of a posterior cerebral artery results in contralateral hemianopia (loss of sight or reduction in vision in one half of the visual field) and contralateral hemisensory loss (loss of sensation on one side of the body). Vertebral artery occlusions can result in nystagmus, dysarthria and diplopia (features of a brain stem lesion) or cerebellar signs such as in coordination and ataxia.
Lacunar Strokes
Lacunar Strokes arise from occlusion of small branches of the anterior and posterior circulation vessels. Different signs can show different lesions although they cannot be fully determined until a CT scan has been performed. Motor hemiparesis usually shows a lesion in the internal capsule however motor hemiparesis with cerebellar type ataxia can indicate a lesion at the posterior internal capsule, midbrain or pons. Hemisensory loss of superficial sensation usually indicates thalamic lesions.